Medical monitoring for eating disorders in NZ involves a structured protocol where General Practitioners and specialists regularly assess vital signs, cardiac function, and blood chemistry to prevent life-threatening complications. This process includes tracking weight restoration, monitoring for refeeding syndrome, and managing electrolyte imbalances caused by malnutrition or purging behaviors.
What Are the Cardiac Risks Associated with Eating Disorders?
The cardiovascular system is often the most severely compromised organ system in individuals suffering from eating disorders, particularly Anorexia Nervosa and severe Bulimia Nervosa. In the context of the New Zealand healthcare system, cardiac complications are the primary driver for urgent hospital admissions within Te Whatu Ora (Health New Zealand) facilities.
When the body is subjected to starvation or severe energy deficits, the heart muscle (myocardium) begins to atrophy much like skeletal muscle. This leads to a reduction in cardiac mass and a decrease in the heart’s ability to pump blood efficiently. The body, in an attempt to conserve energy, lowers the metabolic rate, resulting in significant changes to heart rate and blood pressure.

Why is Bradycardia a Critical Warning Sign?
Bradycardia, defined as a resting heart rate of fewer than 60 beats per minute (bpm), is a common physiological adaptation to malnutrition. However, in the context of eating disorders, it can become dangerous. In New Zealand clinical guidelines, a heart rate dropping below 40 bpm is often considered a “red flag” requiring immediate medical stabilization or hospitalization.
It is crucial to distinguish between athletic bradycardia (seen in high-performance athletes) and pathological bradycardia caused by starvation. In an eating disorder patient, a low heart rate is not a sign of fitness; it is a sign that the heart is struggling to function with limited fuel. Alongside bradycardia, patients often present with hypotension (low blood pressure) and orthostatic changes—a significant drop in blood pressure upon standing, which can lead to fainting (syncope) and falls.
How Do Electrolyte Imbalances Affect the Heart?
Electrolyte disturbances are frequently seen in patients engaging in purging behaviors (vomiting, laxative misuse, or diuretic abuse) and can lead to sudden cardiac arrest. The primary electrolytes of concern include:
- Potassium (Hypokalemia): Low potassium levels destabilize the electrical activity of the heart, leading to arrhythmias (irregular heartbeats). This is a medical emergency and requires immediate correction, often via intravenous fluids in a hospital setting.
- Sodium (Hyponatremia): Often caused by excessive water loading (drinking too much water to suppress appetite or manipulate weight) or purging. Severe hyponatremia can lead to seizures and coma.
- Magnesium and Phosphate: Deficiencies in these minerals further compromise cardiac function and muscle strength.
How Does Malnutrition Lead to Bone Density Loss and Osteoporosis?
One of the most silent yet enduring physical complications of eating disorders is the impact on skeletal health. Unlike some soft tissue damage, bone density loss is not always fully reversible, making early medical monitoring for eating disorders in NZ essential for long-term quality of life.
During adolescence and early adulthood, the body builds “peak bone mass.” Eating disorders interrupt this critical window. The mechanism involves hormonal suppression; specifically, the hypothalamus reduces the production of sex hormones (estrogen in females, testosterone in males) to conserve energy. This state, known as hypogonadotropic hypogonadism, mimics menopause and accelerates bone resorption while slowing bone formation.
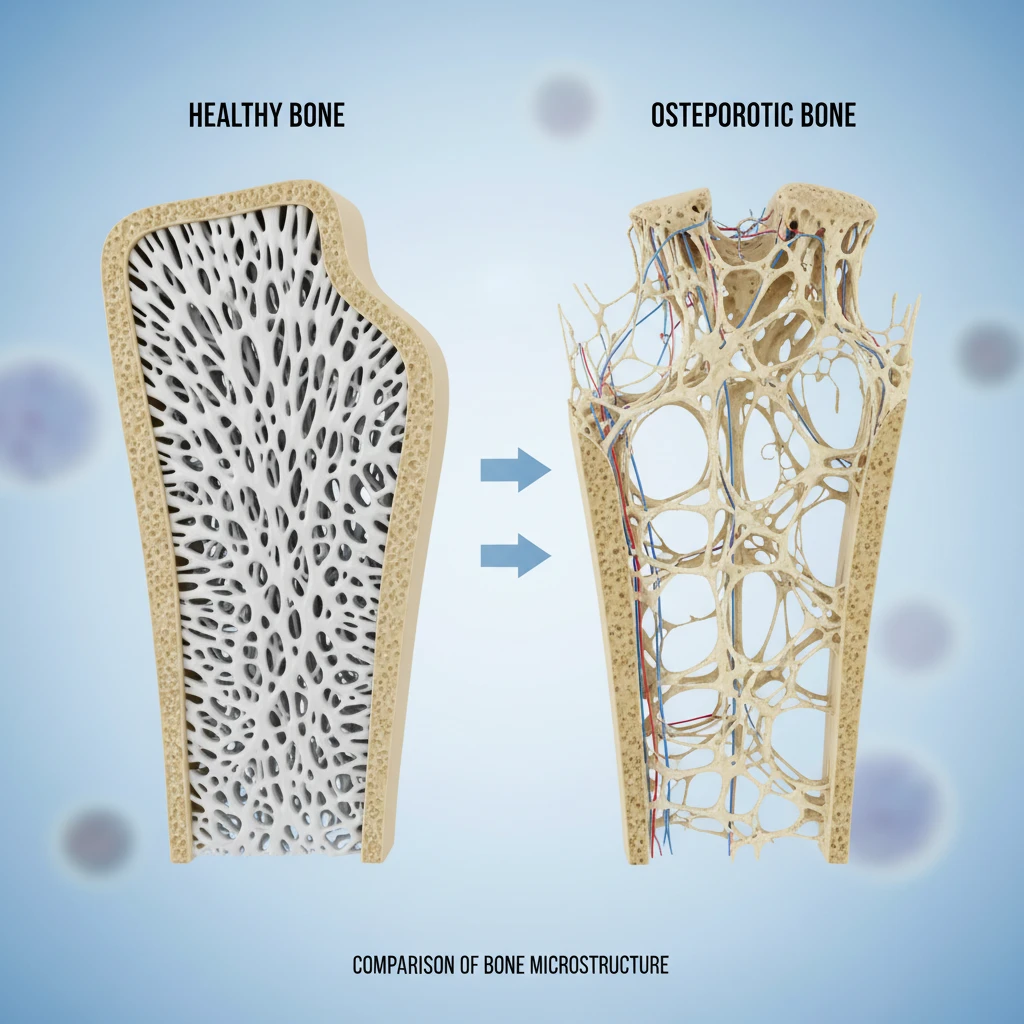
What is Osteopenia vs. Osteoporosis?
Osteopenia refers to lower-than-normal bone density that is not yet severe enough to be classified as osteoporosis. Osteoporosis involves brittle, fragile bones prone to fracture. In the New Zealand context, patients with a long history of amenorrhea (loss of menstrual period) or significant weight loss are typically referred for a DEXA (Dual-Energy X-ray Absorptiometry) scan to assess bone mineral density.
Recovery of bone health is complex. While weight restoration and the resumption of menstruation (or hormonal normalization in males) are prerequisites for halting bone loss, they do not guarantee the complete restoration of lost bone mass. This underscores the importance of prompt intervention. GPs in NZ may prescribe calcium and Vitamin D supplementation, but these are supportive measures and cannot replace the necessity of nutritional rehabilitation.
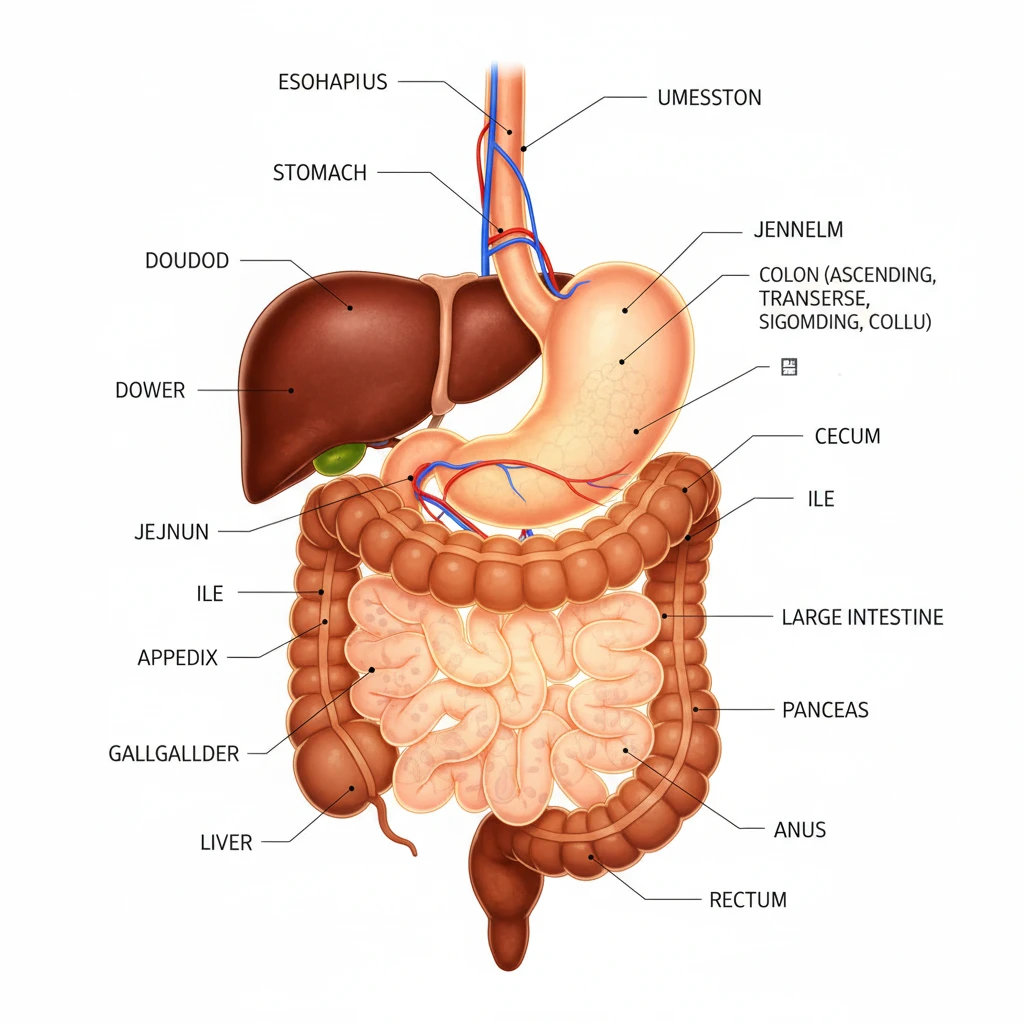
What Are the Gastrointestinal Complications of Eating Disorders?
The digestive system is highly sensitive to nutritional intake. When food intake is restricted, the digestive tract slows down to conserve energy. This leads to a condition known as gastroparesis, or delayed gastric emptying.
What is Gastroparesis?
Gastroparesis occurs when the stomach takes too long to empty its contents into the small intestine. This happens because the stomach muscle atrophies and the vagus nerve, which controls digestive contractions, may not function optimally due to malnutrition. Symptoms include:
- Early satiety (feeling full after a few bites).
- Significant bloating and abdominal distension.
- Nausea and vomiting.
- Abdominal pain.
This creates a vicious cycle in recovery: the patient needs to eat to recover, but eating causes physical pain and bloating, which reinforces the psychological fear of food. It is vital for patients and families to understand that this discomfort is a physiological symptom of starvation, not a sign that the body “doesn’t need” food.
How is Digestive Distress Managed During Recovery?
In NZ treatment settings, dietitians and GPs work together to manage these symptoms. Strategies often include:
- Small, Frequent Meals: Eating smaller amounts more often to reduce the load on the stomach.
- Low Fiber Initially: While fiber is healthy, it slows digestion. Reducing fiber temporarily can help alleviate bloating.
- Metoclopramide: In some cases, medication may be prescribed to stimulate stomach motility.
Crucially, as nutrition is sustained, the digestive muscles regain strength, and gastroparesis typically resolves.
What Are the GP Guidelines for Medical Monitoring in NZ?
In New Zealand, General Practitioners (GPs) play a pivotal role as the primary medical monitors for patients with eating disorders, often acting as the bridge between community care and specialist services. The “Management of Eating Disorders in Primary Care” guidelines provide a framework for assessment and safety.
What Does Routine Monitoring Include?
For a patient with an active eating disorder, medical monitoring is not a one-off event but a regular requirement. The frequency depends on the severity of the illness but often involves weekly or bi-weekly appointments. Standard protocols include:
- Vital Signs:
- Temperature: Hypothermia (body temperature < 35.5°C) is common due to loss of insulating body fat and lowered metabolic rate.
- Pulse & Blood Pressure: Measured sitting and standing to check for postural tachycardia (increase in HR > 20bpm) or postural hypotension (drop in BP > 10-20 mmHg).
- Blood Tests (Phlebotomy):
- Full Blood Count (FBC): To check for anemia and immune function (leukopenia).
- Urea and Electrolytes (U&E): Assessing kidney function, hydration status, and critical electrolyte levels (Potassium, Sodium).
- Liver Function Tests (LFTs): Liver enzymes can be elevated in starvation due to hepatic autophagy (the liver breaking down its own cells for fuel).
- Glucose: Hypoglycemia is a risk, particularly in the morning.
- ECG (Electrocardiogram): To check for QTc prolongation (a delay in the heart’s electrical system increasing risk of arrhythmia) and other abnormalities.

When is Hospitalization Required in NZ?
New Zealand guidelines, such as those referenced by Starship Clinical Guidelines and regional DHBs (now Te Whatu Ora), have specific admission criteria. While clinical judgment is paramount, hospitalization is generally indicated if:
- Weight is less than 75% of expected body weight (or rapid weight loss in adolescents).
- Heart rate is < 40-50 bpm or significant postural changes are present.
- Temperature is < 35.5°C.
- Potassium is < 3.0 mmol/L or other severe electrolyte imbalances exist.
- There is acute refusal of food or fluids leading to immediate medical instability.
What is Refeeding Syndrome?
Refeeding Syndrome is a potentially fatal metabolic complication that can occur when nutrition is reintroduced to a severely malnourished patient. It is one of the primary reasons why “medical monitoring for eating disorders NZ” is so critical during the initial stages of recovery.
How Does Refeeding Syndrome Occur?
During starvation, the body switches from using glucose for energy to using fatty acids and muscle protein. This leads to a depletion of intracellular minerals, although blood levels may appear normal because the body pulls these minerals out of cells to maintain blood homeostasis.
When feeding begins, insulin is released to process the carbohydrates. Insulin drives glucose, potassium, magnesium, and phosphate into the cells to produce energy. If the body’s stores are depleted, blood levels of these minerals drop rapidly (especially phosphate), leading to heart failure, respiratory failure, and seizures.
Prevention and Management
To prevent this, refeeding is started “low and slow” under strict medical supervision. Prophylactic phosphate and thiamine (Vitamin B1) supplementation are standard practices in NZ hospitals to protect the brain and heart during this metabolic shift. Blood tests are conducted daily during the first week of refeeding to monitor these levels closely.
Neurological and Cognitive Impact
While often categorized as a mental illness, the physical impact of eating disorders on the brain is profound. The brain consumes roughly 20% of the body’s dietary energy. In a state of famine, the brain physically shrinks (pseudo-atrophy). This is evidenced by enlarged ventricles and widened sulci on MRI scans.
This structural change manifests functionally as:
- Cognitive Rigidity: Difficulty switching tasks or adapting to new rules (obsessive behaviors).
- Poor Concentration: Inability to focus on school or work.
- Emotional Dysregulation: Heightened anxiety, irritability, and depression.
The encouraging news is that research suggests these structural changes are largely reversible with sustained weight restoration and maintenance. The brain is resilient, but it requires consistent fuel to repair itself.
Frequently Asked Questions
How often should bloods be checked for an eating disorder?
The frequency of blood tests depends on the severity of the illness and the risk of refeeding syndrome. In high-risk patients or those actively purging, bloods may be checked weekly or even daily in a hospital setting. For stable outpatients, monthly monitoring or monitoring coinciding with medication reviews is common. Your GP will determine the schedule based on NZ clinical guidelines.
What is the cutoff for hospitalization for eating disorders in NZ?
While criteria vary slightly by region, general thresholds for admission in New Zealand include a heart rate below 40 bpm, blood pressure below 80/50 mmHg, temperature below 35.5°C, severe electrolyte imbalance (e.g., Potassium < 3.0 mmol/L), or rapid weight loss combined with food refusal. Mental health risk (suicidality) is also a key factor.
Can heart damage from anorexia be reversed?
In many cases, yes. The heart muscle is capable of regaining mass and function once nutrition is restored and a healthy weight is maintained. Bradycardia and hypotension typically resolve with weight restoration. However, chronic damage, such as mitral valve prolapse related to muscle atrophy, may persist, necessitating long-term cardiac monitoring.
What are the symptoms of electrolyte imbalance?
Symptoms can range from mild to life-threatening and include muscle weakness, cramps, palpitations (feeling your heart skip a beat), dizziness, confusion, and extreme fatigue. If you experience these symptoms, especially if you have been purging, seek immediate medical attention.
Do I need a referral for specialist monitoring in NZ?
Yes, typically your GP will refer you to specialized Eating Disorder Services (EDS) within the public health system (Te Whatu Ora) if you meet the criteria. However, your GP remains responsible for physical medical monitoring while you wait for specialist assessment or if you are managed in the community.
How does purging affect electrolytes?
Purging via vomiting causes a loss of stomach acid, leading to metabolic alkalosis and a loss of potassium and chloride. Laxative abuse typically causes a loss of bicarbonate and potassium, leading to metabolic acidosis. Both behaviors dangerously disrupt the electrical balance required for the heart to beat correctly.